At resident report last week Dr. Sonia Godbole presented a case of a patient with a history of IV drug use who was admitted with cellulitis and later developed a recurrent fever and a rash. After a thorough workup he was diagnosed with acute retroviral syndrome (primary HIV). The patient initially tested negative for HIV by the HIV-1/2 + p24 antigen test, but was subsequently found to have a very high HIV viral load and a positive HIV-1/2 + p24 Ag test when re-tested approximately two weeks after admission. The patient likely acquired HIV days before admission, and the initial test was performed in the period before the HIV p24 antigen or HIV antibodies were detectable. As we will review below, this pattern of laboratory tests is consistent with the diagnosis of acute HIV!
This case was a great opportunity to review the different tests for HIV and the timeline of each of the components:
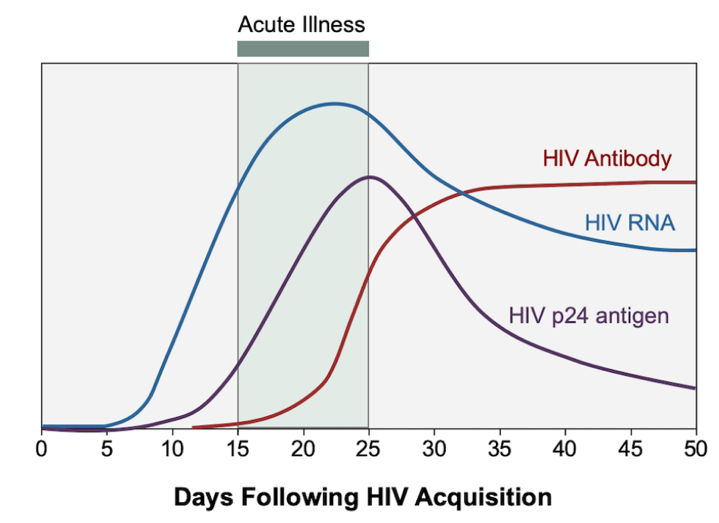
- Approximately 10 days after initial infection the HIV RNA becomes detectable by NAT and quantities begin to increase to very high levels. Acute retroviral syndrome often correlates with the high viral load, though patients can also be asymptomatic.
- The p24 antigen becomes detectable via 4th generation immunoassays 4-10 days after the HIV RNA is detectable
- HIV antibodies are detectable 1 week after the p24 antigen. IgM is detectable ~3 weeks after infection, whereas IgG is positive 4-5 weeks after infection.
- Since the p24 antigen is detectable at least 1 week before HIV antibodies, combined antigen-antibody immunoassays can catch acute infection 1 week earlier than antibody testing alone!
- The window period is the time between initial infection and seroconversion (the first detection of antibodies). For our patient above, the initial assay was performed during this period since neither the p24 antigen nor HIV antibodies were detectable.
- The CDC diagnostic algorithm for acute HIV says to start with the HIV-1/2 antibody + p24 antigen immunoassay (catches 80-85% acute HIV infections). If you have a high clinical suspicion for very early HIV and a negative immunoassay, the next step would be to check HIV RNA.
References:
- Centers for Disease Control and Prevention Association of Public Health Laboratories. Laboratory testing for the diagnosis of HIV infection: updated recommendations. June 27, 2014.
- Cohen MS, Shaw GM, McMichael AJ, Haynes BF. Acute HIV-1 Infection. N Engl J Med. 2011;364(20):1943-1954. doi:10.1056/NEJMra1011874
- Wood BR. Acute and Recent HIV Infection. National HIV Curriculum. September 19, 2020. Accessed November 20, 2020. www.hiv.uw.edu/go/screening-diagnosis/acute-recent-early-hiv/core-concept/all.