On Tuesday Dr. Danielle Kubicki presented a case of a young female w/ no significant PMH presenting with fevers, transient left sided weakness, and R. flank pain. CT imaging revealed a renal infarct. The reason for this infarct (and previous left sided weakness) became clear when blood cultures grew strep mitis. TTE did not reveal any vegetations but since clinical suspicion for infective endocarditis (IE) was high, TEE was pursued which revealed a large mitral valve vegetation with perforation of the anterior leaflet. This patient had no known previous deformity of her mitral valve and no history of recent dental work or tooth abnormality was found.
Danielle taught the surgical indications for left sided native valve infective endocarditis which include the following:
- Signs and symptoms of heart failure from valve dysfunction
- IE complicated by heart block, annular or aortic abscess, or destructive penetrating lesions
- IE caused by fungi or resistant organisms
- Evidence of persistent infection (>5-7 days of bacteremia) after start of appropriate antibiotic therapy
- Recurrent embolic events and persistent or enlarging vegetations despite appropriate antibiotic therapy
- Severe valve regurgitation and mobile vegetations (>10mm), particularly when the anterior leaflet is involved
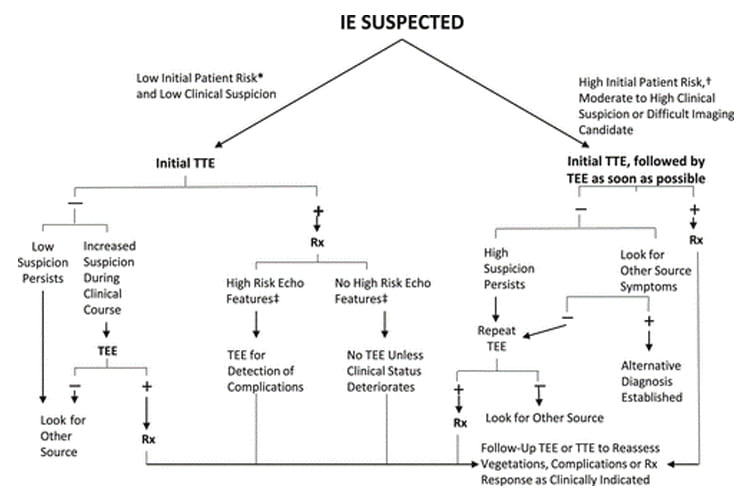
Danielle’s patient was set for the OR due to severe regurgitation with involvement of the anterior leaflet. This case also brings to light the utility of TEE when clinical suspicion for endocarditis is high. Sensitivity of TTE for endocarditis is 70% and approaches 50% when prosthetic valves are involved (due to artifact). Sensitivity for TEE approaches 95% for diagnosing endocarditis.
References:
Wang A, Gaca JG, Chu VH. Management Considerations in Infective Endocarditis: A Review. JAMA. 2018;320(1):72-83. doi:10.1001/jama.2018.7596
Baddour LM et.al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management Complications. Circulation. 2015;132:1435-1486. doi: 10.1161/CIR.0000000000000296