Last week Dr. Hunter Cochran presented a great case of a patient with newly diagnosed renal cell carcinoma and depression who presented with acute encephalopathy in the setting of suspected drug use. On admission the neuro exam was notable for hyperreflexia and bilateral lower extremity clonus. The patient was found to have serotonin syndrome from concomitant use of an SSRI and methamphetamine (which Hunter reminded us is serotonergic!). The patient was started on cyproheptadine and clinically improved.
Hunter had some great teaching points about how to recognize serotonin syndrome:
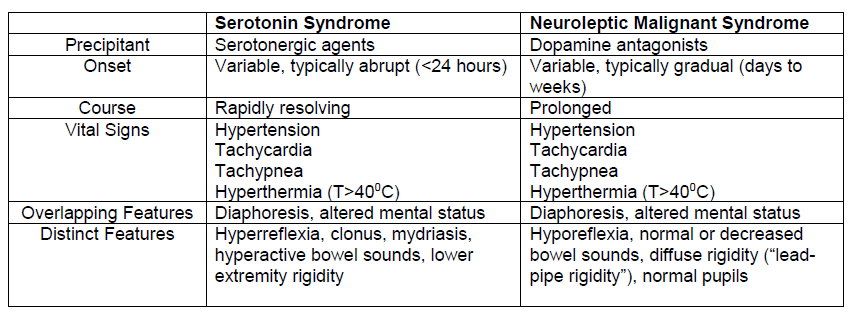
Serotonin syndrome (SS) and neuroleptic malignant syndrome (NMS) are often confused, but each have distinguishing features
Serotonin syndrome is a clinical diagnosis. There are several different diagnostic criteria available for serotonin syndrome, but the Hunter Criteria is considered to be the most accurate and is well validated with 84% sensitivity and 97% specificity!

To fulfill the Hunter Criteria a patient must have taken serotonergic agent AND meet one of the illustrated clinical criteria (Cooper et al.). The Hunter Criteria really emphasizes clonus in the diagnostic criteria, which serves as a great reminder to do a good neuro exam when patients are altered!
_____________________________________________________________________
References:
Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352(11):1112-1120.
Cooper, J., Newby, D., Whyte, I. et al. Serotonin toxicity from antidepressant overdose and its association with the T102C polymorphism of the 5-HT2A receptor. Pharmacogenomics J 14, 390–394 (2014).
Dunkley EJ, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The Hunter Serotonin Toxicity Criteria; simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003;96(9):639.
Perry PJ, Wilborn CA. Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management. Ann Clin Psychiatry. 2012;24(2):155-162.